
| In this article, I make no personal judgements as to the efficacy of Electro-convulsive therapy. It is not the purpose of this talk to address these questions, nor am I qualified to do so. As a medical electronics engineer, it is my responsibility to ensure that the equipment I work on is safe and functioning in compliance with the required standards. |
There are few pieces of equipment in a hospital that evoke such strong opinions amongst the public as the Electro-Convulsive Therapy Machine.
ECT has a poor reputation. This is probably a consequence of its negative portrait in media, and its misuse in public institutions, combined with a general lack of understanding of its use by the public in general. Jack Nicholson’s portrait of ECT in ‘One Flew Over The Cuckoo’s Nest’ left a permanent scar on the memory of a generation who saw the movie. In this 1963 movie, the main character, Randall McMurphy, gets sent to the ‘shock-shop’ as a consequence of his insubordination.

More recently, here in New Zealand, a Royal Commission of Inquiry has recently been hearing details of how ECT was used at the former Lake Alice Psychiatric Facility. The stories of how the ECT machine was used by Doctor Selwyn Leeks, for both convulsive and non-convulsive therapy for the purpose of behavioural modification on children, are the subject of these hearings. The testimonies of how ECT was used at Lake Alice presented at the inquiry are absolutely horrific.
In my electronics workshop, there are few machines that create discussion like an ECT machine when it’s brought in for service. I have been party to many conversations amongst my colleagues regarding these machines and consequently, I tend to avoid servicing ECT machines in my workshop. That way, I can avoid the discussions that ensue over their efficacy.
| “An independent review was conducted in 2003 investigating the safety and efficacy of ECT in New Zealand. The review concluded that ECT continues to have a place as a treatment option available to New Zealanders and that banning its use would deprive seriously ill patients of a potentially effective treatment.” Robyn Shearer, Deputy Director General, Mental Health and Addiction |
What is ECT?
ECT, or Electro Convulsive Therapy, is a medical procedure where the patient has an alternating voltage placed across their skull. The purpose of this voltage is to induce an epileptic seizure in the patient. This seizure is vital to the effectiveness of the procedure. We shall learn why shortly.
A history.
In the late 1800s, early asylum keepers recognised that the symptoms of psychotic patients who also suffered from epilepsy seemed to improve following a seizure. There was also a belief, since disproven, that Epilepsy and Schizophrenia were mutually exclusive, or antagonistic, in patients. This led to the question; could seizures be harnessed as a form of treatment? Whilst this may sound bizarre or even inhuman, these discussions were had at a time when such therapies as fever therapy, lobotomies and insulin comas were considered viable treatments. This was a time when the only alternative to these extreme therapies was permanent institutionalisation.
In 1934, a Hungarian Scientist Ladislas Meduna conducted experiments to discover different ways to induce seizures in patients. One discovery was that the use of the drug, Metrazol produced seizures if administered in high enough doses. Scientists noted that a patient’s psychotic symptoms did diminish after a Metrazol-induced seizure, and this therapy became known as convulsive therapy. However, there were unfortunate side effects, such as convulsions so violent that a study at New York State Psychiatric Institute found that 43% of patients undergoing this form of therapy experienced fractures in their vertebrae. Also, Metrazol induced such feelings of dread in the patients during the brief period following administration, that patients would violently resist follow-up therapy.
Consequently, scientists looked for alternative ways to induce seizures.
An Italian professor of neuropsychiatry, Ugo Cerletti, had been looking into this issue. There is a story that says that Cerletti stopped by the butcher one day on his way home from work. The butcher did not have the cut of meat that Cerletti requested, so the butcher led Cerletti out to the slaughterhouse. The butcher took a pair of electrodes and connected them to the head of a live pig to stun the animal prior to slitting its throat. Cerletti watched the animals’ violent convulsions and wondered if the same shocks could be used to induce seizures in human patients. This led to him experimentally causing seizures in dogs by delivering elect shocks to their heads.
Despite the objections of his colleagues, in 1938 Cerletti called upon his colleague, Lucino Bini to build the first device designed to explicitly deliver therapeutic shocks to humans, which he then tried on his first patients. It worked just as Cerletti had hoped, the shock anaesthetised the patient so that when they woke, they had no memory of the seizure. And the patient showed marked improvement upon waking, as with Metrazol. Beginning in the 1940s, Cerletti and Bini’s technique, dubbed ‘electroconvulsive therapy’ or ‘ECT’, was adopted by almost every major psychiatric institution around the world. ECT was a welcome replacement for Metrazol therapy, as it was less expensive, less frightening to patients, less dangerous (no more broken bones), and more convenient and effective.
Depressed patients showed dramatic improvement, and while there were still side effects of ECT, they were much less than those associated with such therapies as coma therapy, malaria therapy or lobotomies. It was considered a miracle treatment by many.
Early ECT was administered in ’unmodified’ form, which is a euphemistic way of saying that psychiatrists did not use anaesthesia or muscle relaxants. Consequently, full-scale convulsions could still produce bone fractures. Muscle relaxants combined with a short-acting anaesthetic are now used when ECT is applied.
ECT Today
Modern ECT is a relatively simple, straightforward procedure. The patient goes into the therapy room (often wearing their own clothes). Therapy and monitoring electrodes are applied to the patient’s head. A short-acting anaesthetic and muscle relaxant are then applied (sufficient to stop the violent jerking that has historically caused injuries but still enable the patient to have a seizure) and an alternating electrical impulse, ranging from 3-8 seconds is applied. The seizure typically lasts 20-30 seconds. The anaesthetic then wears off, and the patient is awake about 15 minutes later.
ECT in New Zealand
| “ECT machine makers have admitted that their machines can cause permanent memory loss and brain damage. I was harmed, have permanent memory loss, and like many others in my support group cannot function well enough to keep a job, but ACC refused me cover for that injury, while the Minister of Health says it’s safe and effective. I feel it condemns people harmed by ECT to a life in poverty stuck on a benefit”.Petition of Malcolm Richards: End Electroconvulsive Therapy (ECT), July 2020. |
A petition to the house of representatives in 1999 to ban ECT resulted in the commissioning of a comprehensive review of the efficacy and safety of treatment in New Zealand. Despite the review determining that the use of ECT was safe and effective, the government is still regularly petitioned to stop its use, the most recent (at the time of writing) being in July 2021.
At the time of writing, there are 22 ECT machines in use in New Zealand. The most common model appears to be the Somatics Thymatron, followed by the Mecta Spectrum.
| Auckland District Health Board | 2 |
| Canterbury District Health Board | 4 |
| Capital Coast District Health Board | 2 |
| Counties Manukau District Health Board | 1 |
| Hauora Tairawhiti (Gisborne) | 0 |
| Hawkes Bay District Health Board | 1 |
| Hutt Valley District Health Board | 1 |
| Lakes District Health Board | 1 |
| Mid-Central District Health Board | 2 |
| Nelson Marlborough District Health Board | 1 |
| Northland District Health Board | 2 |
| South Canterbury District Health Board | 0 |
| Taranaki District Health Board | 1 |
| Wairarapa District Health Board | 0 |
| Waitemata District Health Board | 2 |
| Waikato District Health Board | 2 |
| West Coast District Health Board | 0 |
| Whanganui District Health Board | 0 |
Compared to other countries, New Zealand has a relatively low rate of therapy per capita population. In 2017, the most recent statistics I have access to, 265 people received ECT, resulting in 2914 treatments. This averages eleven administrations of ECT per patient.
How do they work?
The earliest models of ECT machines were relatively simple, consisting of two independent circuits:
- A low-voltage DC circuit for measuring the patient’s head resistance
- An AC circuit, consisting of an autotransformer with an output of 50-150 VAC, and a timer switch, to create the therapy voltage output.

Tracy Gough Machine, dated 1943. Constructed in Christchurch by Leonard Johns of Gough’s. Johns stated, “It was my own design from top to bottom.” The only knowledge he had of how to construct such a unit was a description in the British Medical Journal dated 1939, which he said, ‘was not much good’. Due to the war, there was a scarcity of parts at the time of construction. The machine had a good success rate and was used for over 20 years before being dumped in a farm pit, from which it was later recovered.
Since the early days of ECT, a lot of experimentation has been done to establish what waveforms, frequencies and durations would provide optimal results and better outcomes.
The most popular model used in New Zealand is the Thymatron System 4.
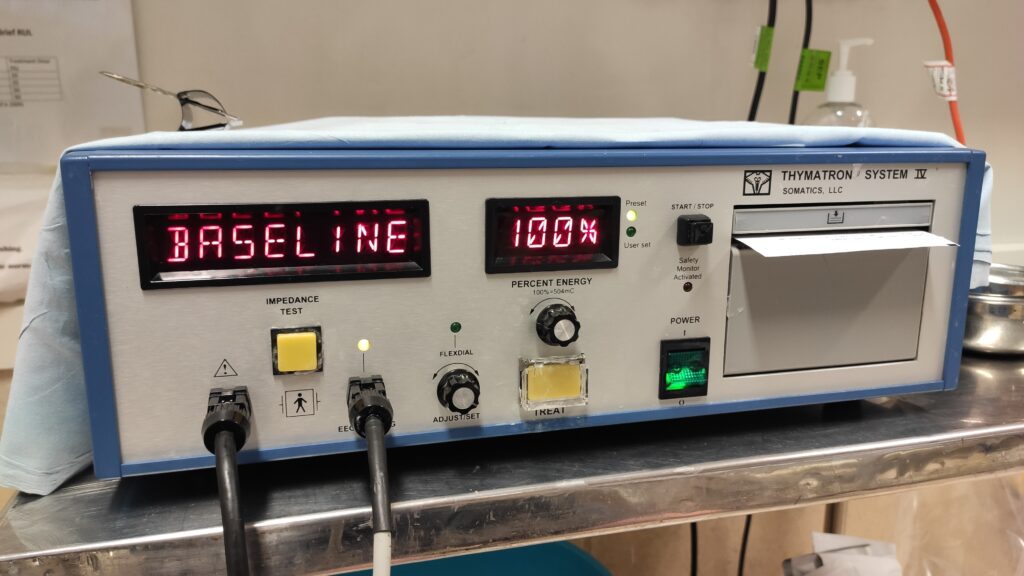
The Thymatron System IV is the most popular ECT Therapy machine in New Zealand.
This machine consists of the following:
Percentage Energy display
- Power switch
- Impedance/Time display
- Therapy Cable Output.
- Monitoring Cable Input: This is used for monitoring the patient’s ECG, EEG or EMG input. This can be printed and used by the machine to determine seizure quality.
- Impedance Test Button: Pressing this button will display the patient’s impedance across the skull between pads. The machine will not deliver a therapy output if the impedance exceeds 3000 Ohms.
- Dose Adjustment Dial: Output is set in percentage, i.e., 10% is equal to 10 Joules.
- Flexdial: For the setting of machines parameters
- Integrated printer: Used for printing therapy results.
- Treat Switch
The System 4 has 7 stimulus programs built in, however, the operator can manually select individual parameters, such as output frequency or pulse width and duration. Manufacturers usually state a ‘first dose’ setting, and depending on the result of initial therapy, clinicians can titrate therapy as required for further treatments.
Output is measured in coulombs, which is a measure of current over time. This figure is used to quantify the total stimulus or ‘dose’.
Current (A) x pulse width (milliseconds) x frequency (Hz) x time (Seconds) x 2 (if biphasic)
Treatment output varies widely; a young female may require 50mC to reach the seizure threshold, whereas an elderly man may require more than 700mC.
The user manual contains charts detailing durations and energy outputs for various programs and frequencies.
An example of this is if the machine is set to a frequency of 60Hz, and the power dial set to 5%, the patient will receive 25.2 mC, or 5 joules of energy. At 100%, the patient will receive 504mC or 99.8 Joules of energy.
The actual output varies as per the user settings. The clinician can adjust the frequency and duration of the biphasic square wave output however, the machine is a fixed-current machine, meaning that it will try to deliver and maintain a current of 0.9 A. This means that if a patient’s head has a high resistance, the machine will increase its output voltage up to 450 Volts to overcome the resistance.
Interestingly, Joules is a product of Voltage (V) x Current (I) x Time (Seconds). Therefore, if the maximum output of the machine is 100 Joules; this is enough to power a 100W electric light bulb!
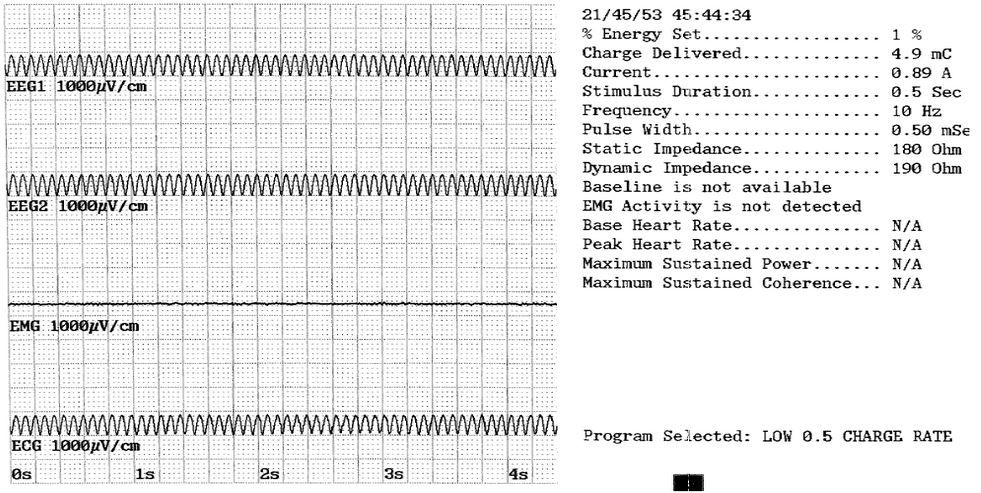
This is a printout following a 1% treatment. The waveforms to the left are generated by a function generator, and on the right, a breakdown of the applied energy. Notably, 1% energy, delivering 4.9mC at .89A.
Conclusion:
I hope that you have found this introduction interesting. The ECT machine is a fascinating device with a dark and much-maligned history. Some patients swear by it, whilst others claim it ruined their lives. However, given the current state of New Zealand’s mental health, its usage continues to increase, and it’s certain to be around for a while yet.
